第一對神經-嗅神經
1.解剖生理
|
|
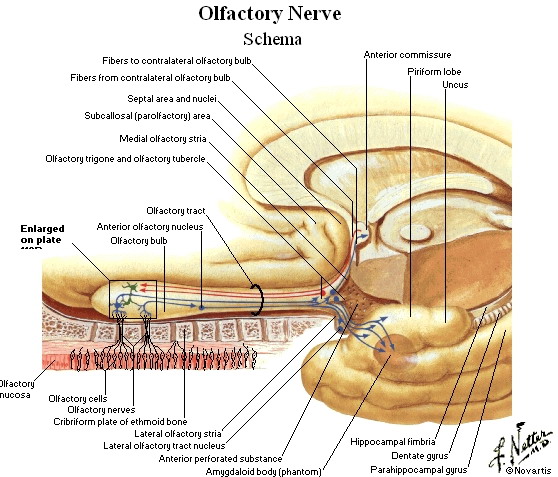
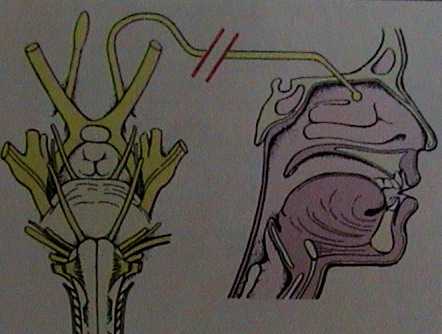
嗅神經為腦神經解剖最復雜的一對。鼻腔上部嗅黏膜中的雙極嗅神經元,中樞支集合成約20個小支,
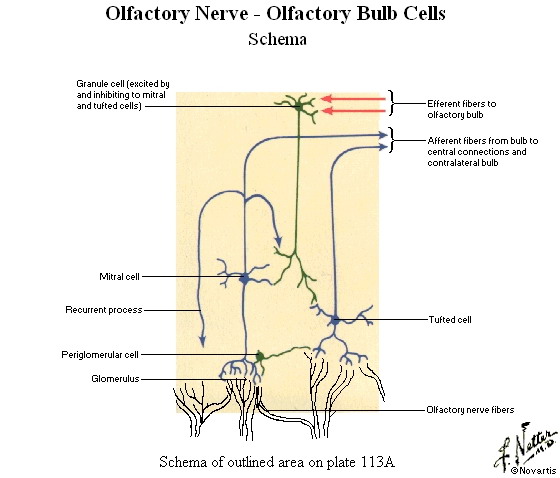
穿過篩板和硬腦膜,終止于嗅球,由這20個小支構成嗅神經。由嗅球的第二級神經元發出縴維經嗅束、
外側嗅紋終止于嗅中樞,即顳葉的鉤回、海馬回的前部及杏仁核。經內側嗅紋及中間嗅紋的縴維分別
終止于胼胝體下回及前穿質與嗅覺的反射聯絡相關。
2.檢查
 |
Cranial nerve I is the olfactory nerve that mediates the sense of smell. it is probably the least tested of the cranial nerves and the least helpful in neurotogc diagnosis because of ts vutnerabIity to a wide range of influences, such as rhinitis. craniotacia! trauma. and smoking. Olfactory function is easily tested.
Present a common substance below one nostril while closing ofl the other,
and ask the patient to identify the odor. For best results, use a substance
|
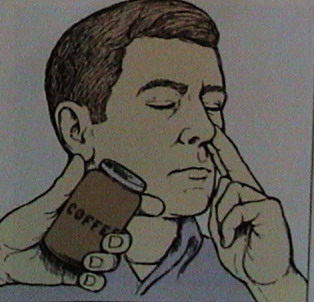 |
先詢問病者有無主觀嗅覺障礙,後讓病人閉上眼楮,分別檢查兩側鼻孑L,非受試側鼻孔以手指堵閉,
用盛有各種揮發氣味的溶液(如松節油、薄荷水、玫瑰水等)的小瓶,或用有氣味的香皂、牙膏、香煙等物,
分別置于病人受檢的鼻孔,要求其說出聞到的氣味或物品。
3.臨床意義
嗅覺障礙常由鼻腔病變引起,感冒及鼻炎等時多為雙側性的。無鼻腔疾病,單側嗅覺減退或缺失較雙側更有臨床意義,
多見于嗅溝腦膜瘤、前顱凹骨折等。在顳葉海馬回病變刺激時則可出現幻嗅。海馬在解剖上靠近垂體和視交叉,
垂體瘤、鞍上囊腫(顱咽管瘤)、視交叉膠質瘤、顳葉腫瘤與顳葉外傷瘢痕可引起鉤回發作,病人可有嗅幻覺,
或伴有味幻覺、夢樣狀態、咂嘴、下頜嚼動、吞咽或全身抽搐。