第二對神經-視神經
解剖生理
|
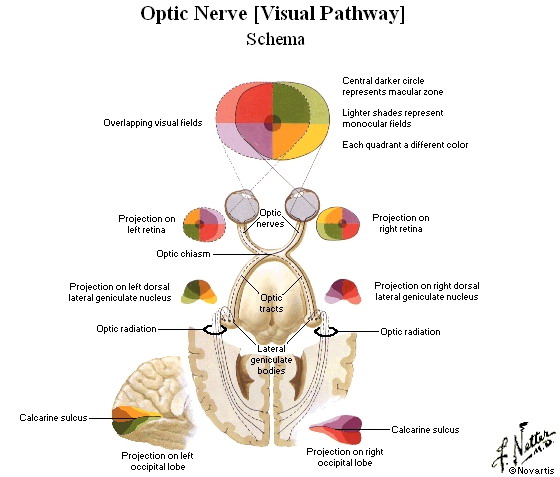
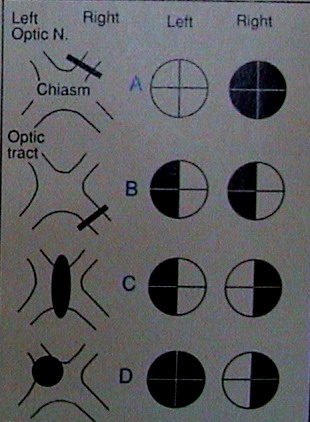
視覺通路為眼球的視網膜、視神經、視交叉、視束、外側膝狀體、視輻射及枕葉視覺皮層。視網膜為視覺感受器,
是眼球壁最內層,主要由四層細胞構成,這四層細胞從外到內是色素上皮細胞層、視桿細胞及視錐細胞層、雙極細胞層、
視網膜神經節細胞層。視桿細胞、視錐細胞是光線感受器,前者位于視網膜周邊部,與周邊部視野有關,後者集中于黃斑中央窩,
與中央部視野(視敏度)有關。視神經起于視網膜神經節細胞層,來自視網膜鼻側半的縴維,經視交叉交叉後,與對側眼球視網膜
顳側半的縴維組成視束,止于外側膝狀體,在此處換元後發出縴維經內囊後肢後部形成視輻射達枕葉距狀裂兩側楔回和舌回的
視中樞皮質——紋狀區。黃斑的縴維投射于紋狀區的後部,視網膜周圍部的縴維投射于紋狀區的前部。光反射的傳導徑路不經過
外側膝狀體,而是由視束經上丘臂人中腦上丘,與兩側動眼神經核相聯系。
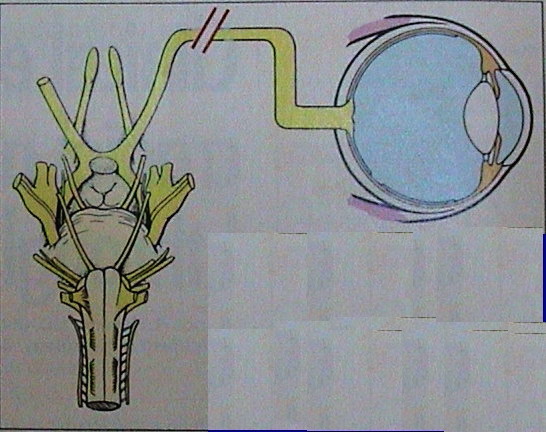 |
Cranial nerve II is the optic nerve
that transmits visual information Its examination includes testing visual acuity and visual fields and performing Fundoscopy. Keep in mind that abnormalities encountered here may also reflect ocular pathology such as corneal disease. cataracts, or retinal lesions. |
檢查
檢查按照以下順序。
(1)視力︰對訴有視力障礙者應用視力表檢查,也可用看書報法粗略測定。如視力減退不能用視力表檢查時,可用指數、指動、
電筒光感測定。光感消失者稱為失明。
 |
The visual acuity of the eyes is best
measured using a standard Snellen distance vision chart at 20 feel. Alternatively, a near vision lest card held at 12 to 14 inches suffices. The goat is to document the best corrected visual acuity, so have the patient who wears eyegLasses or contact lenses wear them during testing or use a 3-diopter magnifying tens. In addition, you can use a pinholo occlude to neutralize many optical causes of diminished visual acuity. |
(2)視野︰為眼楮保持不動位置所能看到的範圍。手試法測定,檢查者與被檢查者相對而坐,相距約60cm,囑被檢查者注視檢查者
相對的眼楮不動(雙方同時用手遮蓋另一眼,病人左手遮左眼,右眼注視檢查者左眼,或反之),檢查者用手指在兩人中間從視野的
外周自上、下、左、右各方逐漸向中心移動,囑病人看見手指時即說出,並與檢查者比較,即可了解視野情況。進一步可用視野計
檢查。
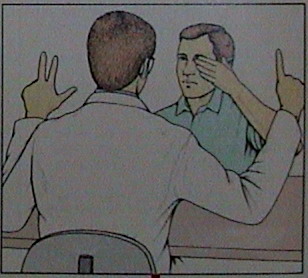 |
Visual fields can be estimated
by using various techniques.One reasonably accurate method involves having the patient cover one eye and focus on your face; with your hands raised to the left and right.Flash different numbers of fingers in two corresponding visual quadrants and ask the patient to state the total number of fingers seen. If.for example, you have presented one finger in the left upper quadrant and two in the right upper quadrant but, on repetition of the exeicise. the patient consistently sees only two fingers, there is probably a left upper field deficit, Follow this procedure for the two lower visual quadrants, and then repeat the sequence in the other eye. |
 |
(3)眼底︰應在不散瞳的情況下進行,以免影響對瞳孔反射的觀察。檢查時要注意觀察視神經乳頭,正常為圓形或卵圓形,淡紅色,
邊緣清楚,中間有生理凹陷。眼底動脈色鮮紅,靜脈色黯紅,兩者管徑的比例為2︰3(A︰V),檢查者要注意視盤的大小、色澤、
形狀、隆起、邊緣。要注意血管的粗細、彎曲度、反光強度及有無交叉壓跡。視網膜有無水腫、出血及滲出物、色素沉著、
結節剝離等。
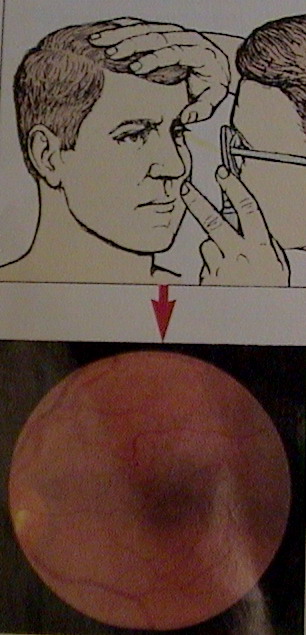 |
Fundoscopic examination allows direct
visualization of important neural and vascular structures. While the patient fixes one eye on a distant point,scrutinize the retina of the other eye for hemorrhages, exudates. and other observable lesions. Next, follow each major retinal vessel to the disc, looking for constriction, dilatation, thickening, sheathing. or bright intravascular objects (atheromatous emboli). Inspect the optic disc for color (normally pinkish yellow).contour(normally flat), and sharpness of margins (normally distinct). Look for spontaneous venous pulsations. Although these pulsations may not be present in healthy individuals, their presence weighs heavily against increased intracranial pressure. Have the patient look at the ophthalmoscope light to bring the macula into view: this area of the retina is normally golden brown or ochre in color and has no vessels. There may be circumstances requiring a specially tailored examination. Sometimes the pupils may have to be pharmacologically dilated. |
臨床意義
1)視神經︰見于視神經本身病變、受壓或高顱壓引起者。視神經病變的視力障礙重于視網膜病變。引起急劇失明多見于眼動脈或
視網膜中央動脈閉塞,視乳頭蒼白,視網膜血管變窄而迂曲,視網膜水腫。數小時或數天達高峰的視力障礙多見于視神經乳頭炎
或球後視神經炎,球後視神經炎常表現急性眼痛,觸診眼球或眼球轉動時明顯。15 9/6∼25%的多發性硬化以球後視神經炎為
首發癥狀。視神經炎多引起中央部視野缺損(中心暗點),視盤水腫多引起周邊部視野缺損及生理盲點擴大。晚期產生繼發性視神經
萎縮,可見進行性視力減退和周邊視野縮小。重度周邊視野缺損稱管狀視野,見于 癥及視覺疲勞。視神經壓迫病變引起不規則
視野缺損,最終產生視神經萎縮及全盲。蝶骨 、嗅溝腦膜瘤可出現腫瘤同側視神經萎縮、對側視乳頭水腫,稱為Foster—Kennedy
征群。
2)視交叉︰視交叉中部受侵犯多引起兩眼顳側偏盲,緣于垂體瘤、顱咽管瘤等的壓迫。一側或兩鼻側偏盲少見,頸內動脈粥樣硬化
壓迫視交叉外側部可產生—側的鼻側偏盲。
3)視束︰一側視束受損,引起兩眼對側視野的同向偏盲,見于顳葉腫瘤或血管病變向內側壓迫時。偏盲側光反射消失。
4)視輻射︰視輻射的下部受損引起兩眼對側視野的同向上象限盲,常為顳葉後部腫瘤或血管病變。視輻射的上部受損兩眼雙側視野的
同向下象限性盲,多為頂葉腫瘤或血管病。視輻射完全受損害時引起兩眼對側視野同向偏盲,見于枕葉腫瘤或大腦後動脈血管病變。
偏盲側光反射仍存在,同時視野的中心部常保存,稱黃斑回避。
5)枕葉視中樞︰病變引起偏盲,並有黃斑回避。枕葉前部受損引起視覺失認。患者不知所見物體的性質和意義。
(2)眼底病變︰
1)視盤水腫︰是一種重要的臨床征象,常見于顱內佔位性病變或炎癥後引起的顱壓增高,如腫瘤、膿腫、血腫、腦出血、
蛛網膜下腔出血、腦膜炎、腦炎、靜脈竇血栓形成等引起顱壓增高時。其發生是由于顱壓增高後影響視網膜中央靜脈和淋巴的
回流所致的。眼底檢查在早期可見視盤充血、邊緣模糊、生理凹陷消失、靜脈淤血,重者視盤隆起可超過2個屈光度,視盤邊緣
完全消失,視盤周圍及視網膜上可有出血。在顱內佔位性病變患者,視盤水腫多在疾病晚期出現,但在生長迅速或很快發生
腦積水的腫瘤患者,視盤水腫出現較早。
視盤水腫需與以下疾病鑒別︰
ヾ視盤炎︰可引起視盤輕度腫脹及靜脈充血,早期迅速表現為明顯視力減退、畏光、眼球運動疼痛,可一側也可兩側。
高顱壓引起的視盤水腫多為雙側的,常比視盤炎所致的嚴重,出血亦比視盤炎多見,早期無視力障礙,視野可正常,
或僅有生理盲點擴大,晚期因繼發性視神經萎縮,視力下降,檢查可發現視乳頭呈蒼白色,動脈細,靜脈怒張大多消退,
邊界模糊不清。球後視神經炎的中心視力很早即發生障礙,如病變位于視神經之前部,可有中度視盤腫脹。
ゝ高血壓眼底改變︰惡性高血壓可有視盤水腫,視盤水腫見于視神經旁,伴有視網膜出血,動脈硬化明顯,管腔狹窄,反光強,
銀絲樣變,靜脈充血不顯著,有動靜脈壓跡。
ゞ假性視盤水腫︰視盤邊緣模糊,為先天性畸形,無水腫和出血,靜脈無怒張,視力正常,無畏光、無眼球痛。
系多量膠質縴維使視乳頭凸出。
2)視神經萎縮︰視神經萎縮可分為原發和繼發兩種。原發性萎縮所見視盤蒼白而境界清楚,篩板清楚,視神經直接受壓、
球後視神經炎慢性期、多發性硬化等脫髓鞘病常有此表現等。繼發性萎縮之視盤蒼白但境界不清,不能窺見篩板,見于視盤水腫、
視神經炎、視網膜炎等的後期。外側膝狀體後和視輻射的病變無視神經萎縮表現。